A DRAFT OF THE PATHOLOGICAL DEMAND AVOIDANCE – BELIEFS SCALE (PDA-BS).
Introduction.
This blog post is an expanded debate entry I have started on Researchgate about a tool to assess a person’s beliefs when they are involved in Demand Avoidance Phenomena (DAP, sometimes called Pathological Demand Avoidance) research. This is the latest draft of the tool and have been constantly revising for over 15 months. There are now 17 questions and a score out of 85. I would greatly appreciate feedback on the tool.
Rationale.
DAP is commonly viewed as part of the autism spectrum, although it is also argued DAP may be either a form of attachment disorder or personality disorder (Woods, 2019). DAP receives significant attention on social media from caregiver campaigning. Despite this interest surrounding DAP it is not a recognised mental disorder construct in the 2 main diagnostic manuals, and it is not universally diagnosed across the United Kingdom (Russell, 2018). The evidence based for DAP is often poor quality, using only all autistic population samples and is circular in nature, relying upon caregiver reports. Hence, it is difficult to draw much firm conclusions about DAP’s nature as much of its research is open to confirmation bias.
Since 2015, frequently DAP researchers state DAP is part of the autism spectrum or express view it is an ASD, for example see research from Eaton et al (2018). We know from statistics from public petitions and surveys from the PDA Society. For instance, see Russell (2018), that caregivers tend to be highly motivated to support a common outlook on it. DAP caregivers are vulnerable due to psychological pressures they often face and their own high anxiety levels (Woods, 2019). That research based on caregiver responses are open to bias (Malik and Baird, 2018; O’Nions et al, 2018).
Furthermore, that autistic persons and persons with DAP are prone to internalising, there are some studies indicating children with DAP have internalised main DAP discourse. It appears that many DAP researchers, along with potential participants of DAP research are biased towards what DAP is and with reliance on circular poor-quality research for DAP; it is probable that this bias is feeding through into DAP research results. O’Nions et al (2016) acknowledges that clinicians can be on the lookout for DAP, and this would be equally applicable to researchers, research participants and other DAP stakeholders.
Ethically, researchers should attempt to falsify their hypothesis, and research should avoid being designed to support a preconceived notion or belief (Woods, 2019). Thus, to improve the quality of DAP research and subsequently in it, I am drafting a short questionnaire that can be used to assess the bias of researchers and participants. The questions are mainly based on common statements that are accepted to be fact by most DAP supporters, yet if one critically engages with the DAP literature these statements are not as true or valid as they appear to be. For instance, DAP is often viewed to be part of the autism spectrum, but there are non-autistic persons with DAP in research samples and some evidence to support DAP is seen in non-autistic persons (Green et al, 2018; Woods, 2019; Woods, 2020). Furthermore, there seems to be a community of practice that has prematurely formed around the notion that DAP is a form of autism (Woods, 2019), this is despite several fallacies in the logic behind assuming DAP is an Autism Spectrum Disorder (Woods, 2021).
The premature formation of a community of practice on the outlook that DAP is a form of autism is problematic for several reasons, including a lack of engagement with critique in critical scholarship which appears to be valid. Elena Garralda (2003) DAP article made observations that are being supported in the literature, such as how DAP might contain features that are associated with Attention Deficit Hyperactivity Disorder (ADHD). This link is having been supported by recent research results (Egan et al, 2020; Green et al, 2018). Another instance is that features of DAP are hard to reliably measure, like features attributed to Surface Sociability trait (Garralda, 2003); in this example features such as “sense of right or wrong” (whose perspective) and “are afraid of their child, and 16 are afraid for her” (this is highly emotive and does not directly assess proposed deficits in social identity/ pride/ shame) (Newson et al, 2003).
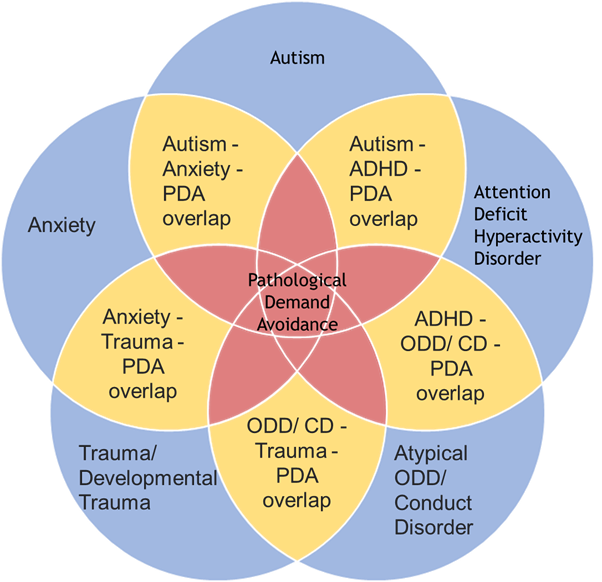
Garralda’s contribution to DAP discourse is frequently overlooked in its literature. For example, I have referenced Garralda (2003) in print more times than (some would argue are leading DAP scholars) Phil Christie and Elizabeth O’Nions combined. It does matter, Richard Soppitt when discussing how DAP relates to other conditions does not mention Garralda’ scholarship when producing the below diagram (Soppitt, 2021, p299):

The above Venn diagram is my edited version of Soppitt’s original image. Not acknowledging Garralda’s input to DAP discourse is reflective of ignoring other critique which appears valid, such as that DAP represents a collection of features from various established conditions (Garralda, 2003; Green et al, 2018; O’Nions et al, 2014b; Woods, 2019). The below Venn diagram displays my interpretation of the literature for what constructs DAP presently overlaps:
Potentially, the most important aspect of DAP that is not widely appreciated in the literature is the sheer number of divergent opinions and conceptualisations of DAP that exists. There are four primarily schools of thought on it:
- Common mental health disorder (Gillberg, 2014).
- Rare autism subtype (Christie, 2007).
- Rebranded autism (Milton, 2017).
- Symptoms from interaction between autism & co-occurring conditions (Green et al, 2018).
For information on these four schools of thought developed, please see this preprint below:
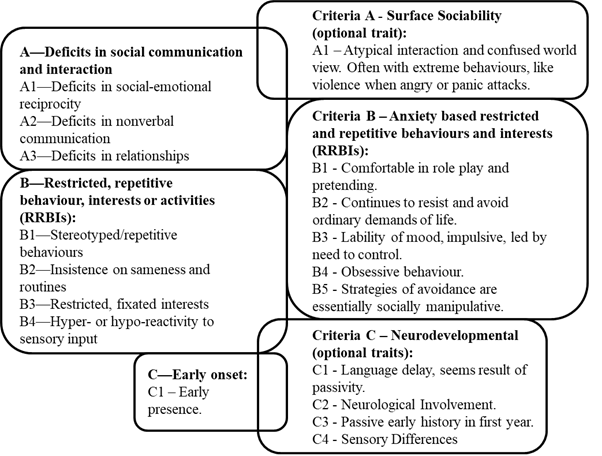
Several different behaviour profiles, see 5 separate profiles, see Eaton et al (2018); Green et al (2018a); Newson et al (2003); O’Nions et al (2016); Woods (2019a). Therefore, I created the aggregated DAP profile to represent divergent opinions on this topic (DSM-5 autism criteria descriptions are from Evers et al, 2021).
These variations in school of thought and behaviour profiles are compounded by how there are several different diagnostic thresholds for DAP, please see the image below.

For a rough guide to these different diagnostic levels, Table 1 shows different properties of the respective diagnostic thresholds.
Table 1: Compulsory features that must be present for various DAP diagnostic thresholds.
| Features need to be compulsory. | DSM-5 OCD. | Eaton and Weaver (2020). | EDA-Q Threshold. | Gillberg et al (2015). | Newson et al (2003). | Wing et al (2011). |
| Demand avoidance ne Pervasive? | No. | Yes. | No. | No. | Yes. | Yes. |
| Demand avoidance from early infancy? | No. | Yes. | No. | No. | No. | No. |
| Person is autistic? | No. | Yes. | No. | No. | No. | Yes |
| Core 5 diagnostic traits present? | Yes. | Yes. | No. | No. | No. | No. |
| Coding issues present? | No. | Yes. | No. | Yes. | Yes. | Unsure. |
For more information on the diagram and these diagnostic thresholds, please see the link below:
One could argue that a leading cause of this myriad of perspectives on DAP, is a lack of adequate engagement with Newson’s original scholarship. We know that Newson was consistent in her view’s DAP is not autism (Newson, 1983; Newson et al, 2003). That she seemingly took steps to ensure DAP not part of the autism spectrum such as including persons who did not meet threshold for either DSM-4 autism subtypes (Christie, 2007) Newson et al, 2003) (It is acknowledged that some in Newson’s cohort do not conform to DSM-5 autism criteria, see Soppitt, 2021). Moreover, persons who displayed autism features, including atypical autism features were excluded from Newson’s DAP database (Newson et al, 2003). I detail most of the steps Newson took to prevent DAP being conceptualised as autism in Woods (2021).
When accounting for the sheer diversity present in outlooks in DAP, that are extant, it is intrinsically unethical to favour a narrow and rigid interpretation of DAP. In my view it is short sighted in the extreme to not adopt a position which is scientific, inclusive and accounts for as many persons with a DAP diagnosis as possible, while not undermining the core traits of DAP (these are approaches I took in outlining my preferred DAP threshold). To quote Judy Eaton:
“Professionals and teams working with children need to become aware of the ways in which girls can mask their difficulties, and need to move away from using the DSM as a ‘bible’. Stating that someone does not fulfil criteria, when these criteria are based on upon a ‘male’ presentation of a disorder, is short sighted in the extreme.” (Eaton, 2017, page 176).
I think these sentiments are equally applicable to conceptualising DAP as part of the autism spectrum. This outlook is supported when key author’s consistently missing/ ignoring non-autistic persons in their research samples (O’Nions et al, 2014a; O’Nions et al, 2015; O’Nions et al, 2016; Reilly et al, 2014). I explain how there is non-autistic persons O’Nions et al, 2014a, in a blog post, I did provide Elizabeth O’Nions with opportunity to provide a robust reason that the CYP with DAP are all autistic and they did not answer. A link to the blog post is below:
https://rationaldemandavoidance.com/2021/04/25/pda-behaviour-intensity-and-prevalance-at-different-thresholds/
Despite repeatedly having non-autistic persons in their DAP research samples, O’Nions has regularly viewed DAP as a form of autism (O’Nions et al, 2014a; O’Nions et al, 2016), and recently (O’Nions et al, 2020; O’Nions & Eaton, 2021). Another example, is Eaton and Weaver (2020) creating their own DAP diagnostic threshold that is not representative of the literature (see the above blog post), as they also used their clinical experience to create their informal DAP algorithm, which is:
“demand avoidance has been present since early infancy and presented across different contexts and time“
“features of the child’s demand avoidance were noted in the child during the assessment process“
“avoidance was pervasive and often seemed illogical or perverse (e.g. the child maybe unable to eat when hungry)“
“avoidance was not limited to a specific activity (or activities) or activities in a specific context (e.g. school)” (Eaton and Weaver, 2020, p37).
One could argue the perception conceptualising DAP as a form of autism is shortsighted is valid and is adversely impacting the quality of its research base. Hence, a robust scientific-method based response is required to counter.
This is only a quick blog post from my perspective and what I recall while typing this blog post; there are other reasons that can be added to strengthen the case for the development and use of the Pathological Demand Avoidance – Beliefs Scale. Persons with DAP deserve better than it being viewed as a form of autism. Autistic persons deserve better than DAP being viewed as a form of autism.
Finally, below I outline the current draft of the PDA-BS and I would appreciate receiving input on it before its empirical validation which should occur late summer/ autumn 2021.
Table 2: Pathological Demand Avoidance – Beliefs Scale (PDA-BS).
| Number | Item | Strongly disagree | Disagree | Neither agree nor disagree | Agree | Strongly Agree |
| 1 | PDA’s other name is Extreme Demand Avoidance. | |||||
| 2 | We need to maintain the integrity of how the condition is understood. | |||||
| 3 | Autistic individuals often benefit from being in control of their lives. | |||||
| 4 | A prolonged debate about what PDA is distracts from focusing on the true purpose of a diagnosis. | |||||
| 5 | The demand avoidance strategies are socially manipulative in nature. | |||||
| 6 | The gender ratio for PDA is evenly split between males and females, it is 1:1. | |||||
| 7 | We need to maintain the integrity of the nature of support that is needed by individuals with PDA. | |||||
| 8 | PDA can be identified in non-autistic persons. | |||||
| 9 | PDA’s primary trait is high anxiety driven demand anxiety. | |||||
| 10 | PDA was a Pervasive Developmental Disorder | |||||
| 11 | Individuals can transition between proposed autism subgroups (e.g. a child diagnosed with more typical autism can grow into the PDA profile). | |||||
| 12 | PDA needs to be significantly different from more traditional autism subgroups (e.g. Asperger’s Syndrome and Kanner’s Syndrome). | |||||
| 13 | PDA has the same strategies and approaches as more typical autism. | |||||
| 14 | PDA is a profile of the Autism Spectrum. | |||||
| 15 | The PDA profile needs to be used all the time with individuals to inform their support strategies. | |||||
| 16 | For PDA, sometimes the demand avoidance is because a person does not want to do an activity. | |||||
| 17 | For PDA, demand avoidance must be present from early infancy, i.e. before 12 months old. | |||||
| Total out of 85. |
Directions of use.
5 Anchor Point scale.
Questions: 1. 2, 4, 6, 7, 9, 10, 12, 14, 15, 17.
(1) Strongly disagree; (2) Disagree; (3) Neither agree nor disagree; (4) Agree; (5) Strongly agree.
Question: 3, 5, 8, 11, 13, 16.
(5) Strongly disagree; (4) Disagree; (3) Neither agree nor disagree; (2) Agree; (1) Strongly agree.
References.
Christie, P. (2007). The distinctive clinical and educational needs of children with pathological demand avoidance syndrome: guidelines for good practice. Good Autism Practice, 8(1), 3–11.
Eaton, J. (2017). A guide to mental health issues in girls and young women on the autism spectrum: diagnosis, intervention and family support. London: Jessica Kingsley Publishers.
Eaton, J., Duncan, K., & Hesketh, E. (2018). Modification of the Coventry Grid Interview (Flackhill et al, 2017) to include the Pathological Demand Avoidant profile. Good Autism Practice, 19(2), 12-24.
Eaton, J., & Weaver, K. (2020). An exploration of the Pathological (or Extreme) Demand Avoidant profile in children referred for an autism diagnostic assessment using data from ADOS-2 assessments and their developmental histories. Good Autism Practice, 21(2), 33-51.
Egan, V., Bull, E., & Trundle, G. (2020). Individual differences, ADHD, adult pathological demand avoidance, and delinquency. Research in Developmental Disabilities. DOI: https://doi.org/10.1016/j.ridd.2020.103733
Evers, K., Maljaars, J., Carrington, S., Carter, A., Happé, F., Steyaert, J.,… Noens, I. (2021). How well are DSM‑5 diagnostic criteria for ASD represented in standardized diagnostic instruments? European Child & Adolescent Psychiatry, 30(2021), 75-87.
Garralda, E. (2003). Pathological demand avoidance syndrome or psychiatric disorder? Archives of Disease in Childhood (online only article). Retrieved from: https://adc.bmj.com/content/88/7/595.responses (Accessed 09 April 2021).
Gillberg, C. (2014). Commentary: PDA – public display of affection or pathological demand avoidance? – reflections on O’Nions et al. (2014). Journal of Child Psychology and Psychiatry, 55: 769–770.
Green, J., Absoud, M., Grahame, V., Malik, O., Simonoff, E., Le Couteur, A., & Baird, G. (2018). Pathological Demand Avoidance: symptoms but not a syndrome. Lancet Child & Adolescent Health, 2(6), 455–464.
Malik, O., & Baird, G. (2018). Commentary: PDA – what’s in a name? Dimensions of difficulty in children reported to have an ASD and features of extreme/pathological demand avoidance: a commentary on O’Nions et al. (2018). Child and Adolescent Mental Health, 23(4), 387–388.
Milton, D. (2017). A Mismatch of Salience: Explorations of the nature of autism from theory to practice. Hove, UK: Pavilion Publishing and Media Limited.
Newson, E. (1983). Pathological Demand-Avoidance Syndrome. Communication, 17, 3-8.
Newson, E., Le Maréchal, K., & David, C. (2003). Pathological demand avoidance syndrome: A necessary distinction within the pervasive developmental disorders. Archives of Disease in Childhood, 88, 595–600.
O’Nions, E., Christie, P., Gould, J., Viding, E., & Happé, F. (2014a). Development of the ‘Extreme Demand Avoidance Questionnaire’ (EDA-Q): preliminary observations on a trait measure for Pathological Demand Avoidance. Journal of Child Psychology and Psychiatry, 55(7), 758–768.
O’Nions, E., Viding, E., Greven, C., Ronald, A., & Happé, F., (2014b). Pathological demand avoidance: Exploring the behavioural profile. Autism, 18(5), 538-544.
O’Nions, E., Quinlan, E., Caceres, A., Tulip, H., Viding, E., & Happé, F. (2015). Pathological Demand Avoidance (PDA): an examination of the behavioural features using a semi-structured interview (Unpublished research). Retrieved from: http://pdaresource.com/files/An%20examination%20of%20the%20behavioural%20features%20associated%20with%20PDA%20using%20a%20semi-structured%20interview%20-%20Dr%20E%20O’Nions.pdf (Accessed 17 January 2021).
O’Nions, E., Gould, J., Christie, P., Gillberg, C., Viding, E., & Happé, F. (2016). Identifying features of ‘pathological demand avoidance’ using the Diagnostic Interview for Social and Communication Disorders (DISCO). European Child & Adolescent Psychiatry, 25(4), 407–419.
O’Nions, E., Viding, E., Floyd, C., Quinlan, E., Pidgeon, C., Gould, J., & Happé, F. (2018). Dimensions of difficulty in children reported to have an autism spectrum diagnosis and features of extreme/‘pathological’ demand avoidance. Child and Adolescent Mental Health, 23(3), 220–227.
O’Nions, E., Ceulemans, E., Happé, F., Benson, P., Evers, K., & Neons, I. (2020). Parenting Strategies Used by Parents of Children with ASD: Differential Links with Child Problem Behaviour. Journal of Autism and Developmental Disorders, 50(2), 386-401.
O’Nions, E., & Eaton, J. (2021). Extreme/‘pathological’ demand avoidance: an overview. Paediatrics and Child Health, 30(12), 411-415.
Reilly, C., Atkinson, P., Menlove, L., Gillberg, C., O’Nions, E., Happé, F., & Neville, B. (2014). Pathological Demand Avoidance in a population-based cohort of children with epilepsy: Four case studies. Research in Developmental Disabilities, 35: 3236–3244.
Russell, S. (2018). Being Misunderstood: Experiences of the Pathological Demand Avoidance Profile of ASD (Online Report). Retrieved from: https://www.pdasociety.org.uk/resources/2018-summary/ (Accessed 16 January 2021).
Soppitt, R. (2021). Pathological/ Extreme Demand Avoidance (PDA/ EDA). In: Peer, L., & Reid, G (Eds.), Special Educational Needs: A Guide for Inclusive Practice (pp. 296-314). London, Sage Publications Limited.
Woods, R. (2019). Demand avoidance phenomena: circularity, integrity and validity – A commentary on the 2018 National Autistic Society PDA Conference. Good Autism Practice, 20(2), 28–40.
Woods, R. (2020). Pathological Demand Avoidance and the DSM-5: a rebuttal to Judy Eaton’s response. Good Autism Practice, 21(2), 74-76.
Woods, R. (2021). Why we should ignore Phil Christie’s views PDA is an Autism Spectrum Disorder (Online video). Retrieved from: https://www.youtube.com/watch?v=GSIdMzDMC-w (Accessed 30 April 2021).

I have made a further revision to this tool.
LikeLiked by 1 person