WHAT DOES AN ETHICAL APPROACH TO PDA LOOK LIKE?
Introduction.
This is a work in progress blog post covering my thoughts on PDA, in relation to its utility, problems with its research, and what an ethical approach to PDA looks like. I have started this blog post in response to being asked these questions. It has motivated me to collate the relevant parts of my various scholarship together in one for ease others access. However, this is a substantial endeavour, it is already at about 4500 words. It is taking longer than I presently have time for. Hence, 2 of the questions need properly fleshing out, the piece needs fully proof reading and fully referenced. I should be able to complete this in significant detail in middle of August 2022. I am making the raw notes publicly available, for ease of others access and to encourage me to finish them when I have time to do. Thinking about this, it might be if the final piece is published across a few blog posts, one for each question to make it manageable for others to read.
Questions.
- To what degree is PDA a useful concept, either from a clinical or research perspective?
- How do you think PDA is being unethically portrayed and propagated?
- What would ethical portrayal look like?
- What is wrong with the current evidence supporting the idea of PDA as a subprofile of autism?
- How, if at all, should researchers and clinicians think of PDA? As a standalone diagnosis? As a personality profile? Something else?
Answers.
To what degree is PDA a useful concept, either from a clinical or research perspective?
- Useful concept for whom? Why is PDA useful?
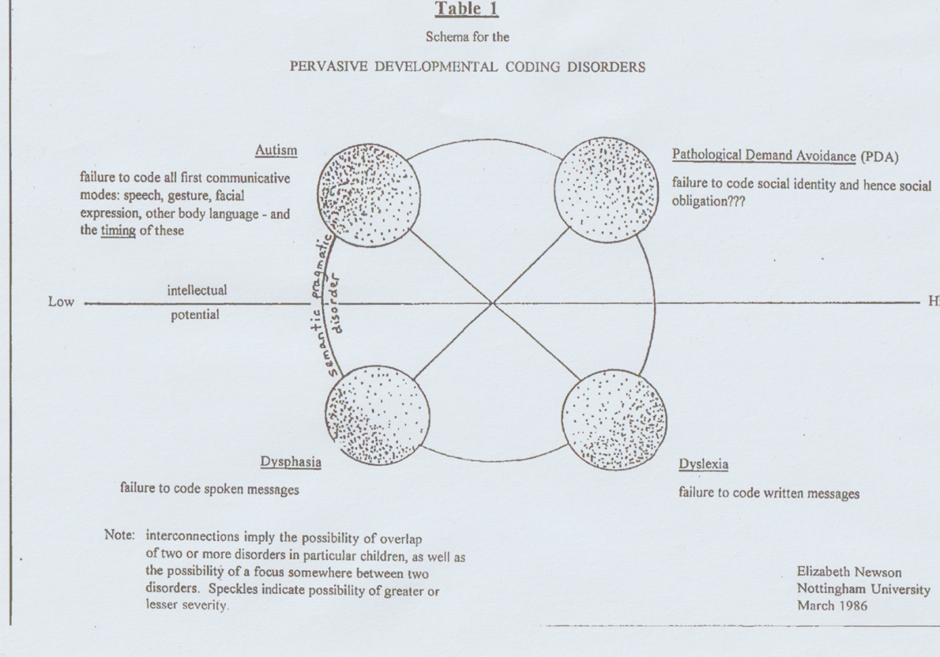
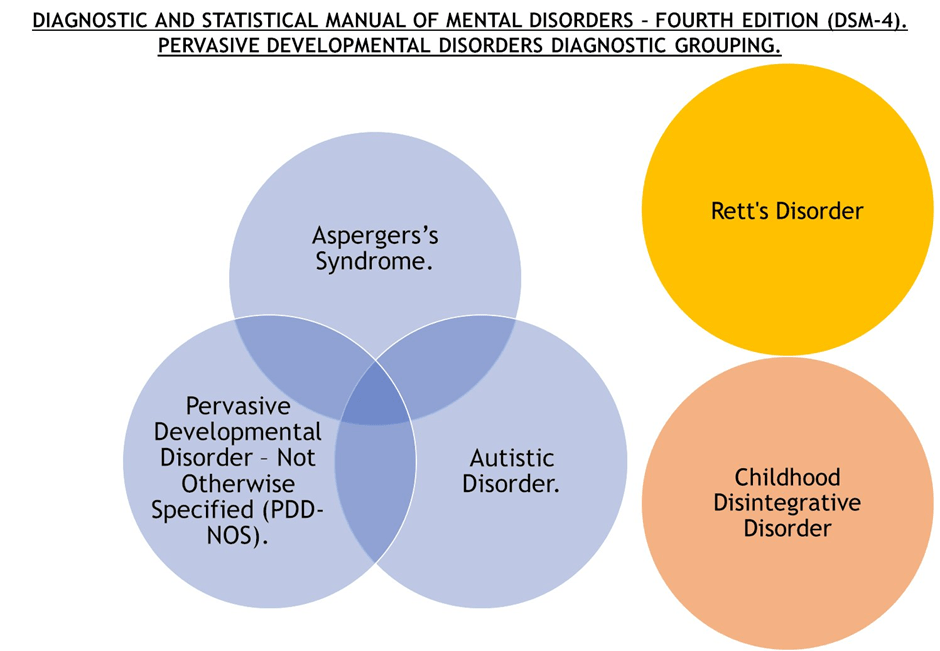
- Mental Disorders are social constructs, no Disorder as described by the DMS-5 has any biomarker evidence that can be used to identify it, and this is not expected to change (Rutter and Pickles, 2016). Rett’s Syndrome was in the same diagnostic grouping as Autistic Disorder & Asperger’s Syndrome in the DSM-4 (APA, 1994). It was removed from the DSM-5 for being associated with a specific biomarker (ref). This means one can create a Disorder and diagnostic groupings out of thin air if they wished to. Newson knew she was reifying PDA when she created her first behaviour profile. Before that, Newson created her own diagnostic grouping for PDA, called Pervasive Developmental Coding Disorders in 1986 (Newson, 1989).
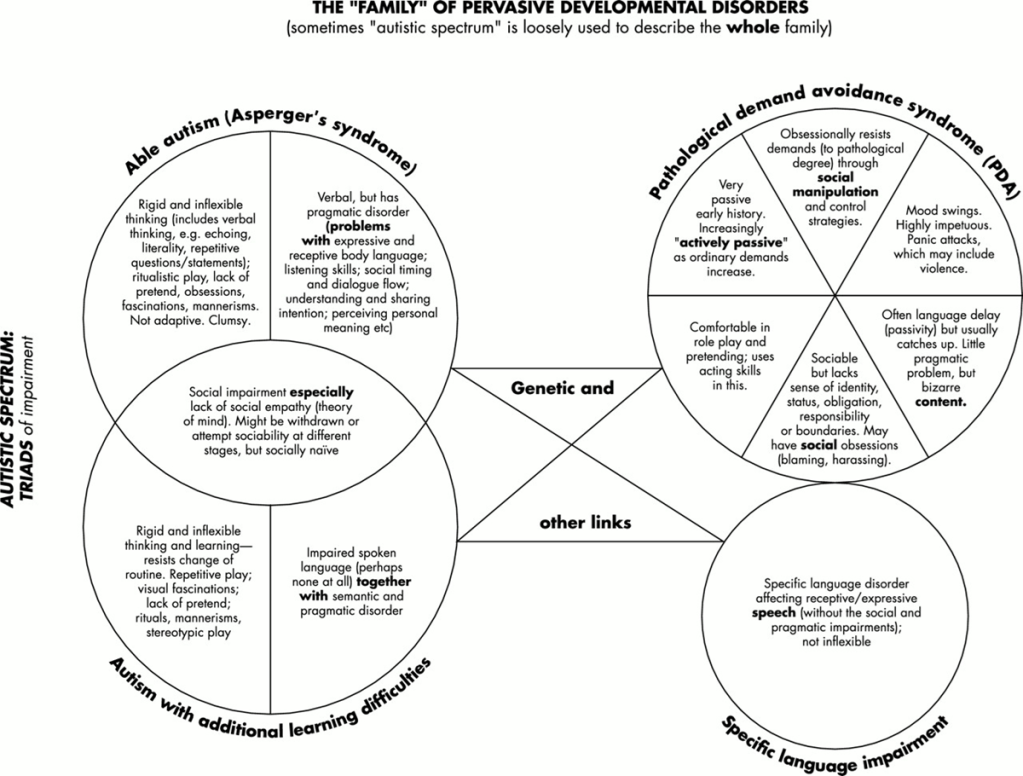
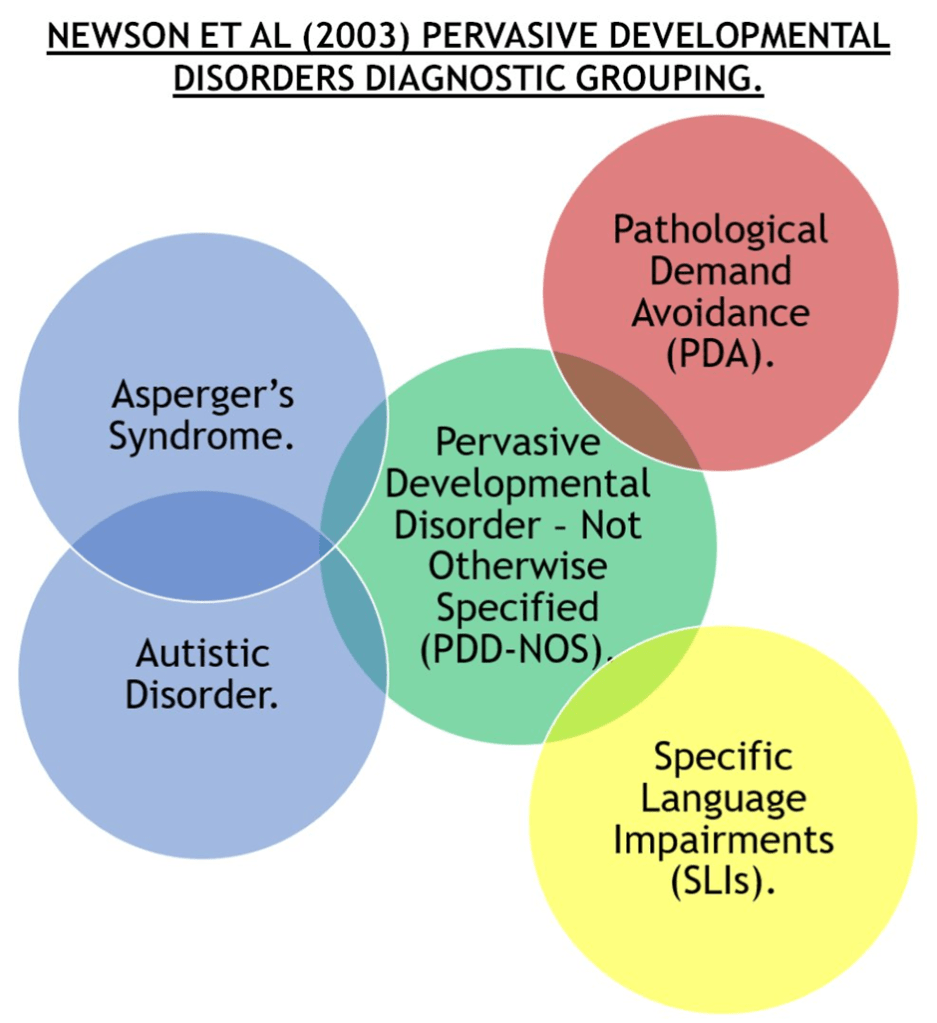
- Later Newson created her version of Pervasive Developmental Disorders diagnostic grouping (Newson et al, 2003, p599). Which is different from diagnostic grouping presented in the DSM-4 (APA, 1994). I will expand upon this later.
- “Like anything else in the social sciences, it depends on how you define and measure it.”. Is my stock response when ask how I am. It is relevant, as there is no consensus over what PDA is, what features are associated with PDA, if PDA should be diagnosed or not, and if so at what diagnostic threshold. The answer to your question is highly subjective. I try to derive my opinion based on typical standards, respecting divergent opinions, PDA and the relevant literature. Overall, I do not think PDA is a helpful concept, but I accept others will disagree with me.
- A diagnosis of a mental Disorder is a long term intervention on a person’s life. Diagnosing someone with autism, ADHD, OCD, BPD, or PDA, can open doors to receiving support, treatments, strategies etc. Giving a person a mental Disorder diagnosis, often changes the quality and quality of opportunities they may encounter often due to stigma of the diagnosis. This is a tangible critique, for PDA there are reports of children with a PDA diagnosis, in the United Kingdom being denied and educational placements. Another example, some clinics in the UK refuse allow persons diagnosed with BPD, access to their services. Any new proposed Disorder needs robust evidence that bestowing a diagnosis of it upon a person, often a vulnerable person, does not adversely affect them; i.e., it must be shown a proposed Disorder like PDA does no harm. We need evidence to inform what is the best way to approach to PDA, that will likely require long term Randomise Control Trials (RCTs).
- PDA is about controlling others, particularly keeping autistic persons under control of others. Much of the PDA discourse is focused on non-compliance of those being attributed PDA.
- PDA is helping some persons, in some aspects. There is supportive community for those who embrace “PDA Profile of ASD”. Why is this community helpful? Many caregivers are exhausted and desperate for something to explain their child’s difficulties and for them to be suitably supported. This creates high power differentials, and it is easy to exploit the caregivers. Generally, people benefit from supportive, like minded communities and positive interactions. PDA researchers report caregivers are highly motivated to take part in their studies (O’Nions et al, 2016b). This is supported by around 1500 persons taking part over two weeks period in the PDA Society’s Being Misunderstood Report (Russell, 2018), and over 10 thousand persons responding to a petition for greater recognition of PDA as a form of autism (ref).
- One of the clinical need arguments for PDA, is that it is needed describe a person’s actions 24 hours a day, so that inform suitable strategies (Christie, 2007). Autistic persons are prone to internalised negative discourses (Woods, 2019). Diagnosing a young child with PDA, is probably an effective way for them to internalise negative discourse surrounding themselves. There are examples of children internalising this discourse surrounding PDA (Woods, 2023).
- It is also useful in controlling researchers and clinicians, as there is substantial hype surrounding PDA, and consistent requests for PDA diagnosis, research and support; there is constant pressure on, organisations, researchers and clinicians to recognise PDA, diagnose and conduct research into PDA.
- Due to sheer diversity of views on PDA and lack of consensus over it. One can reasonably ask, what exactly is being understood when someone is diagnosed with PDA?
- PDA also further commodifies autistic persons, our actions, especially our self-agency (Woods, 2017). Most/ all persons have a need for control, or benefit from being in charge (Woods, 2019). Critical Autism Studies scholars argue PDA represents the pathologising of behaviours people express to assert their self-agency when stressed (Milton, 2017; Moore, 2020; Woods, 2017; Woods, 2019). The “PDA Profile of ASD” narrative is part of broader pattern of behaviour of the autism industry. Provide a horror story which makes caregivers angry and scared about a loss of a normal life. While then selling a product, which gives caregivers hope of a normal life again (McGuire, 2016). In the case of PDA, caregivers are often vulnerable due to issues created by their child often expressing the features of PDA, which are intrinsically difficult for anyone to self-regulate, and others to manage. Hope is sold to caregivers that if their child has a “PDA Profile of ASD” diagnosis, and they campaign for it to be recognised, then their child will be suitably supported, and thus have a normal life again.
- An example of ways PDA is used to control people. There is substantial unhappiness with “Pathological” descriptor of PDA, which has lead to many different names for PDA in print (Woods, 2020). Despite this “PDA Profile of ASD” advocates use a panda as an image for PDA, see the image below:

Giant Pandas have similar connotations attached to them as notions around “PDA Profile of ASD”:
– Are rare.
– Must have campaigning to support their unique needs.
– Have specific approaches which work for them
– Limited space to accommodate them, need to protect how they are understood.
Reinforces certain notions around “PDA Profile of ASD”.
- Some persons do seem to be doing financially well out, and/ or careers are benefitting from “PDA Profile of ASD”.
- I accept that I am part of the PDA Industry, e.g., we are doing this interview…
- Second main argument for PDA’s clinical need is that it has different strategies compared to autism. In this case that those with PDA do not respond well to traditional reinforcement-based approaches for autism (Newson et al, 2003; Christie, 2007; O’Nions and Neons, 2018), i.e., Applied Behavioural Analysis, and Positive Behaviour Support. Issue here is that those approaches are substantially contested, with autistic persons stating they are not effective (Milton, 2013). Recently, in the UK a report has said that Positive Behaviour Support should not be used with autistic persons (Gore et al, 2022). Additionally, non-autistic persons express demand-avoidance features for similar reasons to autistic persons, but are also exposed to reinforcement-based approaches (O’Nions and Neons, 2018). If one takes an inclusive approach to PDA, with a low diagnostic threshold, then surely, PDA is also needed to protect these non-autistic persons with PDA?
- More broadly than this, it is argued that PDA strategies are widely practiced with autistic persons, including evidenced based practices (Green et al, 2018). That there are overlaps with PDA strategies and other common approaches (Woods, 2019). Furthermore, most strategies/ interventions are not diagnostic category specific. It seems ethically problematic to associate strategies which are “common practice” with a one diagnostic category, as is proposed with “PDA Profile of ASD”.
- Autistic persons are no more likely to be involved with criminal justice system than non-autistic persons. Yet, PDA pathologises plenty of criminal behaviours, the below list of behaviours are taken from 11 Revised PDA questions for the Diagnostic Interview for Social and Communication Disorder (DISCO) (O’Nions et al, 2016a):
– screams, has temper tantrums, scratches, bites, kicks or passively resists,
– fails, screams, hits, kicks in a panic tearing up another person’s work, pulling off someone’s spectacles, taking pants down and urinating on floor, injuring someone else’s pet animal
– lie, or cheat, or steal?
– slip from loving to violent behaviour
– frequently tease, bully, refuse to take turns, make trouble harass other people? (e.g. writing threatening letters, making verbal threats, stalking, untrue accusations of sexual abuse). - Autistic persons often adversely affected by stigma by stereotypes, judged, and discriminated by others. Can internalise stigma, more vulnerable to poorer mental health & low self-esteem Can respond to this by concealment and camouflaging, selective disclosure and self-advocacy, as well as positive reframing and reconstructing identity (Han et al 2021). Camouflaging is deleterious to autistic wellbeng (Mandy, 2019). Autistic persons do not need more stigma due to PDA risking associating criminal behaviours with autistic persons.
- PDA stereotypes tend to be opposite of autism stereotypes, as set out in the below table.
Table1: Autism stereotypes and corresponding points from PDA clinical literature.
| Autism Stereotypes. | DAP Clinical Literature. |
| Absent or delayed roleplay and pretend. | Comfortable in roleplay and fantasy.* |
| Are not sociable. | Are sociable, but it is surface. |
| Delays in social communication and interaction from Theory of mind deficits. | Surface sociability, appears to lack of sense of social identity, pride, or shame.* |
| Dislikes surprises. | Likes novelty. |
| Does not express strong emotions. | Intense emotions and dysregulation. |
| Does not make eye contact. | Makes eye contact. |
| Lacks empathy. | Manipulative demand avoidance behaviours.* |
| Likes routines and structure. | Dislikes routines and structure.* |
| Likes routines and structure being imposed upon them. | Has a need for control. |
| Passionate interest with unusual intensity/ focus. | Intense interests are often focused on people. |
| Should use clear and concise language. | Should use complex language to disguise demands. |
| There are many more autistic males, than females. | Female form of autism. Can be equally prevalent in both genders.* |
| Typical autism strategies (often behaviourism based, like Applied Behaviour Analysis) work. | Typical autism strategies (often behaviourism based, like Applied Behaviour Analysis) do not work.* |
*Are reasons why it is problematic conceptualising PDA as an autism subgroup (Woods, 2022).
Those not conforming to autism stereotypes are most likely not to receive an autism diagnosis under DSM-5 criteria (Evers et al 2021). PDA features are opposite of many autism stereotypes, it makes it harder for autistic persons to manage their information.
- No statistical differences in exclusions between Autistic CYP with & without DAP. Few group differences in frequency of failed school placements (Truman et al 2021). PDA diagnoses seem not to making to be making a difference to success rates educational placements and exclusions. There are reports of children diagnosed with PDA being denied an educational placements. Afterall, who would want to have a pupil at their school who has a “pathological”/ “extreme” avoidance to “ordinary” (from others) demands? Likewise, who would want to employ someone who has a “pathological”/ “extreme” avoidance to “ordinary” (from others) demands?
- Most social model neurodiversity supporters do not want autism to be pathologised in the diagnostic manuals like DSM-5 and ICD-11 (Chown & Leatherland, 2018). Pathologises more aspects of autistic persons, not covered in an DSM-5 autism criteria. Keeps autism under control of non-autistic stakeholders.
- Milton (2019) questions what the impact of PDA is on the autistic community? Divides autism, goes against most autistic persons, creates internalised ableism based conflict within the autistic community and broader neurodiversity movements. There is intense debate within the autistic community over PDA, sometimes the debates turn vicious. Below are two examples of memes by a pro “PDA Profile of ASD” support which attack myself and Damian Milton.
- Fundamentally, we stopped using autism subtypes as all attempts to successfully divide autism have failed, or differences are due to circular practices., i.e., how one designs and measures autism subtypes (Woods, 2020). Recent efforts to create subgroups, such as PDA and “Profound Autism” use co-occurring difficulties to divide autistic persons into subgroups (Woods, 2021). Furthermore, the many statistics indicating how bad autistic persons are suffering from lack of suitable support (Botha, 2021; Woods, 2017); means it can be said all autistic persons are “complex”. Yet, such issues should already be covered by specifiers in DSM-5. Treating PDA as an autism subgroup reifies nonsensical notions that there are “typical”/ “normal” “straight-forward” cases of autism.
- There is growing unease with use of Mental Disorders, and good case to stop using, such as by Kinderman (2019). DSM-5 recognises present classification system is a stop-gap until something better comes along (APA, 2013). Move towards transdiagnostic approach (Astle et al 2021; other article 2022), instead of Disorders. Treating PDA as an autism subgroup reinforces present paradigm with Mental Disorders and medical model of autism, which seems increasingly problematic and likely to be swept away in a paradigm shift.
- A couple of recent studies are indicating PDA is not a distinct entity (Schneider et al, 2022; White et al, 2022); PDA as a concept has all these severe problems, and it might turn out that PDA is a pseudo-syndrome, i.e., not a distinct Disorder/ Syndrome/ Profile!
- Monotropism is better for viewing autism (Garau, 2022; Murray, 2018).
- I view taking a transactional stress account to be best way to conceptualise PDA as a distinct entity, for instance see this video below:
https://www.youtube.com/watch?v=7cCYoHV4li8
How do you think PDA is being unethically portrayed and propagated?
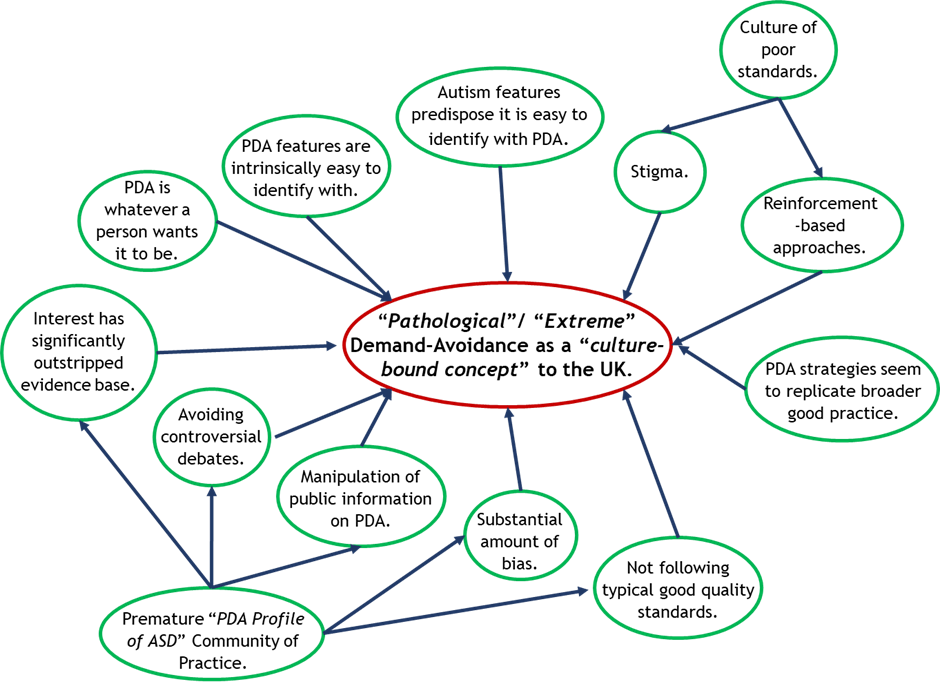
- Bubble should not exist…
- Poor quality ethics and poor quality research and practice go hand in hand (Waltz, 2007).
- Power differentials. Ethical duty to provide balanced and accurate information.
- Ignoring anything mildly inconvenient, e.g., citation survey results (Woods, 2019).
- Eaton & Weaver (2020) example.
- If there was a robust ethical case for “PDA Profile of ASD”, it would have been made by now…
- COI pushing a particular outlook,
- It is horrifically circular, ignoring far to many inconvenient things (which is discussed in the next session) to justify doing.
- Assuming PDA is a “Profile of ASD” biases PDA research and tools against what PDA might look like in non-autistic persons. It is the same circular process which biases the autism diagnostic criteria and tools in favour of white-males. Ironically, some key “PDA Profile of ASD” supporters reasonably point out about not being hide bound to biased autism criteria, e.g., see (Eaton, 2017), but are not open minded to PDA presenting differently to their perspective of PDA.
- The circularity is a problem. If one only diagnoses PDA in autistic persons, only develops tools for PDA in autistic persons and only conducts research of PDA in autistic persons; how we will be able to test competing views on PDA? How can we test if non-autistic persons with PDA exist? How can we test if non-autistic persons with PDA face similar/ same issues as autistic persons with PDA (thus should receive a PDA diagnosis)? How can we respect Disability law, and universal rights of non-autistic persons with PDA?
- PDA Society asked me to share my concerns with PDA, and how they are portraying it. I gave them a detailed and evidence-based reasons for my concerns. They ignored it.
- Not declaring conflict of interests, for example:
https://www.paediatricsandchildhealthjournal.co.uk/article/S1751-7222(22)00046-4/fulltext
- Generally, those in powerful positions advocating for “PDA Profile of ASD”, do not respect or care about divergent opinions, or supporting evidence for divergent outlooks on PDA, there is an unsaid axiom that only “PDA Profile of ASD” supporters know what PDA is and what it looks like.
- Attempting to maintain integrity for “PDA Profile of ASD”.
- Breach universal rights and disability legalisation.
- Ignoring autistic persons preferences. When at a time of respecting autistic persons wishes (supposedly), Identity first, vs person first language.
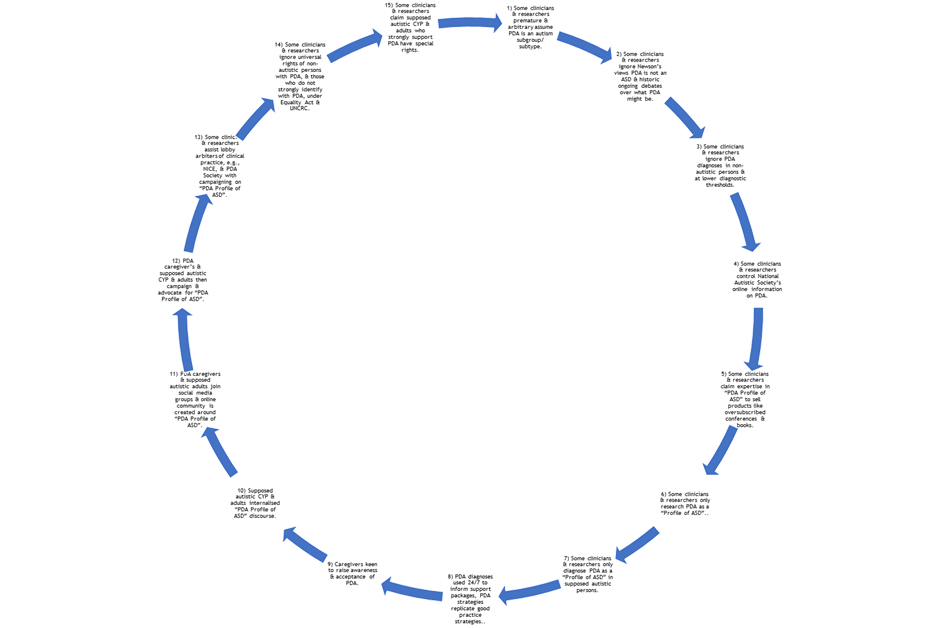
| Number. | Component in creating demand for “PDA Profile of ASD”. |
| 1 | Some clinicians & researchers premature & arbitrary assume PDA is an autism subgroup/ subtype. |
| 2 | Some clinicians & researchers ignore Newson’s views PDA is not an ASD & historic ongoing debates over what PDA might be. |
| 3 | Some clinicians & researchers ignore PDA diagnoses in non-autistic persons & at lower diagnostic thresholds. |
| 4 | Some clinicians & researchers control National Autistic Society’s online information on PDA. |
| 5 | Some clinicians & researchers claim expertise in “PDA Profile of ASD” to sell products like oversubscribed conferences & books. |
| 6 | Some clinicians & researchers only research PDA as a “Profile of ASD”. |
| 7 | Some clinicians & researchers only diagnose PDA as a “Profile of ASD” in supposed autistic persons. |
| 8 | PDA diagnoses used 24/7 to inform support packages, PDA strategies replicate good practice strategies. |
| 9 | Caregivers keen to raise awareness & acceptance of PDA. |
| 10 | Supposed autistic CYP & adults internalised “PDA Profile of ASD” discourse. |
| 11 | PDA caregivers & supposed autistic adults join social media groups & online community is created around “PDA Profile of ASD”. |
| 12 | PDA caregiver’s & supposed autistic CYP & adults then campaign & advocate for “PDA Profile of ASD”. |
| 13 | Some clinicians & researchers assist lobby arbiters of clinical practice, e.g., NICE, & PDA Society with campaigning on “PDA Profile of ASD”. |
| 14 | Some clinicians & researchers ignore universal rights of non-autistic persons with PDA, & those who do not strongly identify with PDA, under Equality Act & UNCRC. |
| 15 | Some clinicians & researchers claim supposed autistic CYP & adults who strongly support PDA have special rights. |
What would ethical portrayal look like?
- I answer this in the last question, because people will portray PDA as they conceptualise it. For instance, a person is not going to portray as a form of attachment disorder, if they conceptualise PDA as a “Profile of ASD”.
What is wrong with the current evidence supporting the idea of PDA as a subprofile of autism?
- There are much which can be said with this. I will start with the axiom that PDA is a “Profile of ASD”, then onto issues measuring PDA, and then discussing some of the methodological limitations, but most methodological limitations are discussed in Kildahl et al (2021) systematic review. There are more fundamental issues, of not following typical standards and ethical values.
- In terms challenging axion PDA is a “Profile of ASD”, there is a lot to discuss. From how Newson conceptualised PDA, through to other arguments that PDA is an ASD. Reasons why it is problematic PDA is an ASD. Finally broader problems trying to divide autism.
- Asperger ignored Sukhareva, & Kanner ignored Asperger. Childhood Schizophrenia is a dead diagnosis used in 1920s – 1980s. Much lack of consensus over what features were in CS. Widely known & diagnosed in CYP, including autistic CYP. Kanner folded autism into CS (Silberman 2015). Newson’s clinic specialised in demographics CS often diagnosed in. Newson collected cases from 1975, when CS was common diagnosis. Newson’s PDA fundamentally same since 1975… What if PDA is based on CS? Would explain Newson’s methodology & axiology.
| Childhood Schizophrenia (Silberman 2015, p341). | Newson et al (2003) PDA Criteria & Descriptions. |
| Gross and sustained impairment of emotional relationships with people. | Lability of mood, impulsive,… Switches from cuddling to thumping for no obvious reason; or both at once. |
| Apparent unawareness of his own personal identity to a degree inappropriate to his age. | Surface sociability, but apparent lack of sense of social identity, pride, or shame. motivation to avoid demands is so sustained, and because the child knows no boundaries to avoidance. Linked to illogical anxiety as in CS trait 6? |
| Pathological preoccupation with particular objects or certain characteristics of them, without regard to their accepted functions. | Obsessive behaviour: Much or most of the behaviour described is carried out in an obsessive way |
| Sustained resistance to change in the environment and a striving to maintain or restore sameness. | Continues to resist and avoid ordinary demands of life. (WITH) strategies of avoidance are essentially socially manipulative. |
| Abnormal perceptual experience (in the absence of discernible organic abnormality). | Comfortable in role play and pretending. |
| Acute, excessive, and seemingly illogical anxiety as a frequent phenomenon. | led by need to control outbursts, screaming, hitting, kicking; best construed as panic attack. Repetitive questions used for distraction, but may signal panic. 60% have extreme outbursts or panic attacks goes “over the top” in protest or in fear reaction. |
| Speech either lost, or never acquired, or showing failure to develop beyond a level appropriate to an earlier age. | Language delay, seems result of passivity. |
| Distortion in motility patterns. | Neurological involvement: Soft neurological signs are seen in the form of clumsiness and physical awkwardness. |
| A background of serious retardation in which islets of normal, near-normal, or exceptional intellectual function or skill may appear. | Unsure, still reflecting upon this one. |
- Check other bullet points.
- INSERT Table comparing the two.
- Expect it to look different in autistic persons, does not mean PDA is a “Profile of ASD”.
- Need evidence to
- It is a self-validation exercise, which is not inclusive, or following typical standards.
- Many studies have severe methodological issues.
- I find the entire axiom PDA is part of the autism spectrum to be harmful nonsense, and I will explain why.
- Childhood Schizphrenia.
- Newson’s axiology and methodology.
- Have it writing PDA was informally excluded from DSM-5 by Neurodevelopmental Disorders Workgroup.
- Reasons PDA is not autism. Including assuming it on a behavioural level, e.g., trauma.
- Subtyping autism problems, including circular nature.
- Demand-Avoidance is transactional stress.
- Problems with underlying definitions.
- Can be diagnosed as a standalone thing.
- Case PDA is seen in non-autistic persons.
How, if at all, should researchers and clinicians think of PDA? As a standalone diagnosis? As a personality profile? Something else?
- Stop pretending PDA is a “Profile of ASD” and diagnosing PDA as a dual diagnosis with autism.
- Stop reifying their own preferred outlook on PDA, over other outlooks. There is no reasonable reason to try and maintain the integrity of PDA, while simultaneously undermining the integrity of autism, and disrespecting most autistic persons preference for autism to be undivided.
- First, one needs to accept the realities in PDA literature and positions of arbiters of clinical practice: there are no consensus over what PDA, what features are associated with PDA, or how to diagnose it and at what diagnostic threshold. Furthermore, there are many ongoing-historic debates with PDA.
- Obviously, there will be different interpretations of the nature of these debates. We should stop misleading the public and the vulnerable persons who are often advocating for PDA, and present these nuanced debates on PDA. This requires being inclusive of, and respecting various competing and diverging outlooks on PDA. It also requires us to respect universal rights of all persons who identify with PDA, like under the United Nations Convention on the Rights of the Child (UNCRC) (Summerhill and Collett, 2018), and associated legal protections, such as from disability legislation, e.g., the UK’s The Equality Act.
- I interpret these overall patterns in PDA’s ongoing-historical debates as its four main school’s of thought (Woods, 2021).
- PDA’s competing hypotheses need to be empirically tested, and with a good evidence base. It is through rigorous investigation of what could PDA be, that various debates surrounding PDA will be resolved. That means as part of these studies, PDA is suitably conceptualised, for example with PDA potentially being a form of personality disorder, it means conceptualising PDA as a personality disorder and empirically PDA as a form of personality disorder. This would include designing suitable tools which assume PDA is a personality disorder.
- This is crucial, as it looks like most competing hypotheses have some evidence, even if is minor, such as PDA as a form of attachment disorder has at least one case of a person with attachment disorder and an ADOS score of one (O’Nions 2013, p226).
- Another example, is in relation to your first question, is PDA a useful concept from a clinical perspective? Surely, that needs long term randomised control trials investigating outcomes of persons diagnosed with PDA, versus persons who receive personalised support packages by assigning PDA’s component features to accepted diagnostic categories; i.e., following process suggested in Green et al (2018).
- While investigating each hypothesis, one can draw multiple different outlooks of PDA. One can test possible clusters of PDA features, for previous reported relationships, such as are there associations with anxiety, conduct problems (Green et al, 2018; O’Nions et al 2014), etc.
- PDA is novel impairment category, anyone interested in PDA should be calling for highest standards possible in PDA ethics, research and practice. That includes large scale RCTs to investigate efficacy of PDA strategies (Woods et al, 2019).
- It also means being mindful of the thresholds we choose for a person having PDA. Most of our research knowledge on PDA involves the EDA-Q. There is no sense to choose a threshold which is substantially divergent from EDA-Q as it means one cannot be reliably sure to generalise EDA-Q derived knowledge (Woods, 2021).
- The wording used in PDA traits often varies from person to person. Some view PDA having social communication issues (Eaton and Weaver, 2020), others do not (Berney et al, 2020). Some view PDA’s lability of mood trait having impulsivity/ hyperactivity, others do not (British Psychological Society, 2022). Some view PDA’s social avoidance behaviours to be manipulative (Gillberg et al, 2015; Newson et al, 2003), others view it to be strategic (O’Nions & Eaton, 2021). This matters as it can also mean that certain tools do not assess features of traits they are purported to (Kildahl et al, 2021).It can also affect how PDA is clinically viewed and thus how a person is treated.
- When talking about PDA, researchers and clinicians need to specific:
- What school of thought they are basing their axiology upon.
- What certain definition for PDA they use.
- What exact behaviour profile they are using, particularly the wording as different versions have different clinical interpretations.
- What their exact threshold for PDA is.
- How would you feel about autistic persons creating a Disorder that pathologises your non-compliance in creating an autism friendly world and lack of empathy towards us? (Woods 2021).
References.
lsdjfksdljfksd
